<link rel="stylesheet" href="http://editor.daum.net/services/blog/css/contents4view.css?ver=1.1.114" type="text/css"/><link rel="stylesheet" href="http://editor.daum.net/services/blog/css/theme4view.css?ver=1.1.114" type="text/css"/><script language="javascript" src="http://pimg.daum-img.net/UX-JS_2008/common_view.js?v=ux5.4"></script><script language="javascript"> var articleno = "110"; </script><A name=01></A>
<H2>Introduction</H2><A id=Introduction name=Introduction></A><A name=0101></A>
<H3>Background</H3><A id=IntroductionBackground name=IntroductionBackground></A>
<P>Arias first described breast milk jaundice (BMJ) in 1963. Breast milk jaundice is a type of <A href="http://emedicine.medscape.com/article/974786-overview" target="_blank"><U><FONT color=#004276>neonatal jaundice</FONT></U></A> associated with breastfeeding. It is characterized by indirect hyperbilirubinemia in a breastfed <A href="http://www.medscape.com/resource/neonatal-medicine" target=_blank><U><FONT color=#004276>newborn</FONT></U></A> that develops after the first 4-7 days of life, persists longer than physiologic jaundice, and has no other identifiable cause. It should be differentiated from breastfeeding jaundice, which manifests in the first week of life and is caused by insufficient production or intake of breast milk.</P><A name=0104></A>
<H3>Pathophysiology</H3><A id=IntroductionPathophysiology name=IntroductionPathophysiology></A>
<P>The etiology of breast milk jaundice is not clearly understood, but the following factors have been suggested to play a role:<BR><BR>
<DIV>
<UL>
<LI>An unusual metabolite of progesterone (pregnane-3-alpha 20 beta-diol), a substance in the breast milk that inhibits uridine diphosphoglucuronic acid (UDPGA) glucuronyl transferase
<LI>Increased concentrations of nonesterified free fatty acids that inhibit hepatic glucuronyl transferase
<LI>Increased enterohepatic circulation of bilirubin due to (1) increased content of beta glucuronidase activity in breast milk and, therefore, the intestines of the breastfed neonate and (2) delayed establishment of enteric flora in breastfed infants
<LI>Defects in uridine diphosphate-glucuronyl transferase (<I>UGT1A1</I>) activity in infants who are homozygous or heterozygous for variants of the Gilbert syndrome promoter and coding region polymorphism.
<LI>Reduced hepatic uptake of unconjugated bilirubin due to a mutation in the solute carrier organic anion transporter protein SLCO1B1.
<LI>Inflammatory cytokines in human milk, especially interleukin (IL)-1 beta and IL-6, are increased in individuals with breast milk jaundice and are known to be cholestatic and reduce the uptake, metabolism, and excretion of bilirubin.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>1</FONT></U></A> </SUP>
<LI>High epidermal growth factor (EGF) levels in breast milk may be responsible for jaundice in these neonates. EGF is responsible for growth, proliferation, and maturation of the GI tract in newborns and is vital for is adaptation after birth. Higher EGF serum and breast milk levels were noted in patients with breast milk jaundice.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>2</FONT></U></A> </SUP>The reduced GI motility and increased bilirubin absorption and uptake are thought to be the mechanisms.</LI></UL></DIV>
<P>Please see <A href="http://emedicine.medscape.com/article/974786-overview" target="_blank"><U><FONT color=#004276>Jaundice, Neonatal</FONT></U></A> for an in-depth review of the pathophysiology of hyperbilirubinemia.</P>
<P></P><A name=0105></A>
<H3>Frequency</H3><A id=IntroductionFrequency name=IntroductionFrequency></A>
<H4>United States</H4><A id=IntroductionFrequencyUnitedStates name=IntroductionFrequencyUnitedStates></A>
<P>Jaundice occurs in 50-70% of newborns. Moderate jaundice (bilirubin level >12 mg/dL) develops in 4% of bottle-fed newborns, compared to 14% of breastfed newborns. Severe jaundice (bilirubin level >15 mg/dL) occurs in 0.3% of bottle-fed newborns, compared to 2% of breastfed newborns. A strong familial predisposition is also suggested by the recurrence of breast milk jaundice in siblings.</P>
<H4>International</H4><A id=IntroductionFrequencyInternational name=IntroductionFrequencyInternational></A>
<P>International frequency is not extensively reported but is thought to be similar to that in the United States.</P><A name=0108></A>
<H3>Mortality/Morbidity</H3><A id=IntroductionMortalityMorbidity name=IntroductionMortalityMorbidity></A>
<P>Breast milk jaundice in otherwise healthy full-term infants rarely causes <A href="http://emedicine.medscape.com/article/975276-overview" target="_blank"><U><FONT color=#004276>kernicterus</FONT></U></A> (bilirubin encephalopathy). Case reports suggest that some breastfed infants who suffer from prolonged periods of inadequate breast milk intake and whose bilirubin levels exceeded 25 mg/dL may be at risk of kernicterus. Another group of breastfed infants who may be at risk of complications are borderline premature infants (36-37 weeks' gestational age) who are poorly nursing.</P><A name=0109></A>
<H3>Race</H3><A id=IntroductionRace name=IntroductionRace></A>
<P>Whether racial differences are observed in breast milk jaundice is unclear, although an increased preval‎!ence of physiologic jaundice is observed in babies of Chinese, Japanese, Korean, and Native American descent.</P><A name=0110></A>
<H3>Sex</H3><A id=IntroductionSex name=IntroductionSex></A>
<P>No sex predilection is known.</P><A name=0111></A>
<H3>Age</H3><A id=IntroductionAge name=IntroductionAge></A>
<P>Breast milk jaundice manifests after the first 4-7 days of life and can persist for 3-12 weeks.</P><A name=02></A>
<H2>Clinical</H2><A id=Clinical name=Clinical></A><A name=0216></A>
<H3>History</H3><A id=ClinicalHistory name=ClinicalHistory></A>
<UL>
<LI>Physiologic jaundice usually manifests after the first 24 hours of life. This can be accentuated by breastfeeding, which, in the first few days of life, may be associated with suboptimal milk and suboptimal caloric intake, especially if milk production is delayed. This is known as breastfeeding jaundice. Jaundice that manifests before the first 24 hours of life should always be considered pathologic until proven otherwise. In this situation, a full diagnostic workup with emphasis on infection and hemolysis should be undertaken.
<LI>True breast milk jaundice (BMJ) manifests after the first 4-7 days of life. A second peak in serum bilirubin level is noted by age 14 days.
<LI>In clinical practice, differentiating between physiologic jaundice from breast milk jaundice is important so that the duration of hyperbilirubinemia can be predicted. Identifying the infants who become dehydrated secondary to inadequate breastfeeding is also important. These babies need to be identified early and given breastfeeding support and formula supplementation as necessary. Depending on serum bilirubin concentration, neonates with hyperbilirubinemia may become sleepy and feed poorly.</LI></UL><A name=0217></A>
<H3>Physical</H3><A id=ClinicalPhysical name=ClinicalPhysical></A>
<UL>
<LI>Clinical jaundice is usually first noticed in the sclera and the face. Then it progresses caudally to reach the abdomen and extremities. Gentle pressure on the skin helps to reveal the extent of jaundice, especially in darker-skinned babies; however, clinical observation is not an accurate measure of the severity of the hyperbilirubinemia.
<LI>A rough correlation is observed between blood levels and the extent of jaundice (face, approximately 5 mg/dL; mid abdomen, approximately 15 mg/dL; soles, 20 mg/dL). Therefore, clinical decisions should always be based on serum levels of bilirubin. Skin should have normal perfusion and turgor and show no petechiae.
<LI>Neurologic examination, including neonatal reflexes, should be normal, although the infant may be sleepy. Muscle tone and reflexes (eg, Moro reflex, grasp, rooting) should be normal.
<LI>Eval‎!uate hydration status by an assessment of the percentage of birth weight that may have been lost, observation of mucous membranes, fontanelle, and skin turgor.</LI></UL><A name=0218></A>
<H3>Causes</H3><A id=ClinicalCauses name=ClinicalCauses></A>
<UL>
<LI>Supplementation of breastfeeding with dextrose 5% in water (D5W) can actually increase the preval‎!ence or degree of jaundice.
<LI>Delayed milk production and poor feeding lead to decreased caloric intake, <A href="http://emedicine.medscape.com/article/906999-overview" target="_blank"><U><FONT color=#004276>dehydration</FONT></U></A>, and increased enterohepatic circulation, resulting in higher serum bilirubin concentration.
<LI>The biochemical cause of breast milk jaundice remains under investigation. Some research reported that lipoprotein lipase, found in some breast milk, produces nonesterified long-chain fatty acids, which competitively inhibit glucuronyl transferase conjugating activity.
<LI>Glucuronidase has also been found in some breast milk, which results in jaundice.
<LI>Decreased uridine diphosphate-glucuronyl transferase (<I>UGT1A1</I>) activity may be associated with prolonged hyperbilirubinemia in breast milk jaundice.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>3</FONT></U></A> </SUP>This may be comparable to what is observed in patients with Gilbert syndrome.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>4</FONT></U></A> </SUP>Genetic polymorphisms of the <I>UGT1A1</I> promoter, specifically the T-3279G and the thymidine-adenine (TA)7 dinucleotide repeat TATAA box variants, were found to be commonly inherited in whites with high allele frequency. These variant promoters reduce the transcriptional <I>UGT1A1</I> activity. Similarly, mutations in the coding region of the <I>UGT1A1</I> (eg, G211A, C686A, C1091T, T1456G) have been described in East Asian populations; these mutations reduce the activity of the enzyme and are a cause of Gilbert syndrome.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>5</FONT></U></A> </SUP>
<LI>The G211A mutation in exon 1 (Gly71Arg) is most common, with an allele frequency of 13%. Coexpression‎! of these polymorphism in the promoter and in the coding region are common and further impair the enzyme activity.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>6</FONT></U></A> </SUP>
<LI>Hepatic solute carrier organic anion transporter 1B1 (SLCO1B1) is a sinusoidal membrane protein involved in uptake of unconjugated bilirubin. Mutation of the gene for SLCO1B1, namely the A388G missense variant, was associated with increased risk of neonatal hyperbilirubinemia with exclusive breast feeding.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>7</FONT></U></A> </SUP></LI></UL><A name=06></A>
<H2>Differential Diagnoses</H2><A id=Differentials name=Differentials></A>
<DIV>
<TABLE class=differentialstable cellSpacing=0 cellPadding=0 border=0>
<TBODY>
<TR vAlign=top>
<TD><A href="http://emedicine.medscape.com/article/780334-overview" target="_blank"><FONT color=#004276><U>Anemia, Acute</U></FONT></A><BR></TD>
<TD><A href="http://emedicine.medscape.com/article/974786-overview" target="_blank"><FONT color=#004276><U>Jaundice, Neonatal</U></FONT></A><BR></TD></TR>
<TR vAlign=top>
<TD><A href="http://emedicine.medscape.com/article/927029-overview" target="_blank"><FONT color=#004276><U>Biliary Atresia</U></FONT></A><BR></TD>
<TD><A href="http://emedicine.medscape.com/article/978352-overview" target="_blank"><FONT color=#004276><U>Neonatal Sepsis</U></FONT></A><BR></TD></TR>
<TR vAlign=top>
<TD><A href="http://emedicine.medscape.com/article/927624-overview" target="_blank"><FONT color=#004276><U>Cholestasis</U></FONT></A><BR></TD>
<TD><A href="http://emedicine.medscape.com/article/957343-overview" target="_blank"><FONT color=#004276><U>Polycythemia</U></FONT></A><BR></TD></TR>
<TR vAlign=top>
<TD><A href="http://emedicine.medscape.com/article/944069-overview" target="_blank"><FONT color=#004276><U>Galactose-1-Phosphate Uridyltransferase Deficiency (Galactosemia)</U></FONT></A><BR></TD>
<TD><A href="http://emedicine.medscape.com/article/976319-overview" target="_blank"><FONT color=#004276><U>Polycythemia of the Newborn</U></FONT></A><BR></TD></TR>
<TR vAlign=top>
<TD><A href="http://emedicine.medscape.com/article/974349-overview" target="_blank"><FONT color=#004276><U>Hemolytic Disease of Newborn</U></FONT></A><BR></TD>
<TD><FONT color=#004276><U></U></FONT></TD></TR>
<TR vAlign=top>
<TD><A href="http://emedicine.medscape.com/article/922777-overview" target="_blank"><U><FONT color=#004276>Hypothyroidism</FONT></U></A><BR></TD>
<TD><U><FONT color=#004276></FONT></U></TD></TR></TBODY></TABLE></DIV><A name=0615></A>
<H3>Other Problems to Be Considered</H3><A id=DifferentialsOtherProblemstobeConsidered name=DifferentialsOtherProblemstobeConsidered></A>
<P>Hemolytic anemia (RBC membrane defects: spherocytosis, <A href="http://emedicine.medscape.com/article/954356-overview" target="_blank"><U><FONT color=#004276>acanthocytosis</FONT></U></A>, ovalocytosis; RBC enzyme defects, hemoglobinopathies)<BR>Blood type incompatibility (ABO and minor group antigens)<BR>Large cephalhematoma<BR><A href="http://emedicine.medscape.com/article/922777-overview" target="_blank"><U><FONT color=#004276>Hypothyroidism</FONT></U></A> <BR><A href="http://emedicine.medscape.com/article/969643-overview" target="_blank"><U><FONT color=#004276>Urinary tract infections</FONT></U></A> <BR><A href="http://emedicine.medscape.com/article/972559-overview" target="_blank"><U><FONT color=#004276>Sepsis</FONT></U></A> <BR>Gilbert syndrome<BR>Early galactosemia</P><A name=07></A>
<H2>Workup</H2><A id=Workup name=Workup></A><A name=0719></A>
<H3>Laboratory Studies</H3><A id=WorkupLabStudies name=WorkupLabStudies></A>
<DIV>
<UL>
<LI>Breast milk jaundice (BMJ) is a diagnosis of exclusion. Detailed history and physical examination showing that the infant is thriving and that lactation is well established are key elements to diagnosis. Breastfed babies should have 3-4 transitional stools and 6-7 wet diapers per day and should have regained birth weight by the end of the second week of life or demonstrate a weight gain of 1 oz/d.
<LI>Measure total serum bilirubin concentration in neonates who have jaundice that has progressed from the face to the chest and in neonates at risk for <A href="http://emedicine.medscape.com/article/974349-overview" target="_blank"><U><FONT color=#004276>hemolytic disease of the newborn</FONT></U></A>.
<LI>The following tests are to be considered if serum bilirubin levels are greater than 12 mg/dL (170 ?mol/L). A total serum bilirubin concentration that rises faster than 5 mg/dL/d (85 ?mol/L/d) or jaundice before 24 hours of life suggests pathologic jaundice.
<LI>A level of conjugated bilirubin greater than 2 mg/dL (34 ?mol/L) suggests <A href="http://emedicine.medscape.com/article/927624-overview" target="_blank"><U><FONT color=#004276>cholestasis</FONT></U></A>, <A href="http://emedicine.medscape.com/article/927029-overview" target="_blank"><U><FONT color=#004276>biliary atresia</FONT></U></A>, or <A href="http://www.medscape.com/resource/sepsis" target=_blank><U><FONT color=#004276>sepsis</FONT></U></A> (see <A href="http://emedicine.medscape.com/article/974786-overview" target="_blank"><U><FONT color=#004276>Jaundice, Neonatal</FONT></U></A>).
<LI>CBC count with reticulocyte count findings are as follows:
<UL>
<LI><A href="http://emedicine.medscape.com/article/957343-overview" target="_blank"><U><FONT color=#004276>Polycythemia</FONT></U></A> (hematocrit level, >65%)
<LI>Anemia (hematocrit level, <40%)
<LI>Sepsis (WBC count, <5 K/mL or >20 K/mL) with immature to total neutrophil ratio greater than 0.2</LI></UL>
<LI>Urine specific gravity can be useful in the assessment of hydration status.
<LI>If hemolysis is suspected, consider the following tests:
<UL>
<LI>Blood type to eval‎!uate for ABO, Rh or other blood group incompatibility
<LI>Coombs test, as well as an elution test for antibodies against A or B, to eval‎!uate for immune mediated hemolysis
<LI>Peripheral smear to look for abnormally shaped RBCs (ovalocytes, acanthocytes, spherocytes, schistocytes)
<LI>Glucose-6-phosphate dehydrogenase (G-6-PD) screen, especially if ethnicity consistent</LI></UL>
<LI>Factors that suggest possibility of hemolytic disease include the following:
<UL>
<LI>Family history of hemolytic disease
<LI>Onset of jaundice before 24 hours of life
<LI>Rise in serum bilirubin levels of more than 0.5 mg/dL/h
<LI>Pallor, hepatosplenomegaly
<LI>Rapid increase in serum bilirubin level after 24-48 hours (G-6-PD deficiency)
<LI>Ethnicity suggestive of G-6-PD deficiency
<LI>Failure of phototherapy to lower bilirubin level</LI></UL>
<LI>If sepsis is suspected, consider the following tests:
<UL>
<LI>Blood culture
<LI>WBC differential
<LI>Platelet count
<LI>Urine analysis and culture</LI></UL>
<LI>Factors that suggest the possibility of sepsis include the following:
<UL>
<LI>Poor feeding
<LI>Vomiting
<LI>Lethargy
<LI>Temperature instability
<LI>Apnea
<LI>Tachypnea</LI></UL>
<LI>Signs of cholestatic jaundice that suggest the need to rule out biliary atresia or other causes of cholestasis include the following:
<UL>
<LI>Dark urine or urine positive for bilirubin
<LI>Light-colored stools
<LI>Persistent jaundice for more than 3 weeks</LI></UL>
<LI>The follow-up includes the state newborn screen for galactosemia and <A href="http://www.medscape.com/resource/hypothyroidism" target=_blank><U><FONT color=#004276>hypothyroidism</FONT></U></A>.</LI></UL></DIV><A name=11></A>
<H2>Treatment</H2><A id=Treatment name=Treatment></A><A name=1127></A>
<H3>Medical Care</H3><A id=TreatmentMedicalCare name=TreatmentMedicalCare></A>
<DIV>
<UL>
<LI>Treatment recommendations in this section apply only to healthy term infants with no signs of pathologic jaundice and are based on the severity of hyperbilirubinemia. In preterm, anemic, or ill infants and those with early (<24 h) or severe jaundice (>25 mg/dL or 430 ?mol/L), different treatment protocols should be pursued (see <A href="http://emedicine.medscape.com/article/974786-overview" target="_blank"><U><FONT color=#004276>Jaundice, Neonatal</FONT></U></A>).
<LI>For healthy term infants with breast milk or breastfeeding jaundice and with bilirubin levels of 12 mg/dL (170 ?mol/L) to 17 mg/dL, the following options are acceptable:
<UL>
<LI>Increase breastfeeding to 8-12 times per day and recheck the serum bilirubin level in 12-24 hours. The mother should be reassured about the relatively benign nature of breast milk jaundice (BMJ). This recommendation assumes that effective breastfeeding is occurring, including milk production, effective latching, and effective sucking with resultant letdown of milk. Breastfeeding can also be supported with manual or electric pumps and the pumped milk given as a supplement to the baby.
<LI>Continue breastfeeding and supplement with formula.
<LI>Temporary interruption of breastfeeding is rarely needed and is not recommended unless serum bilirubin levels reach 20 mg/dL (340 ?mol/L).</LI></UL>
<LI>For infants with serum bilirubin levels from 17-25 mg/dL (294-430 ?mol/L), add phototherapy to any of the previously stated treatment options. The reader is referred to the American Academy of Pediatrics' practice parameter on the management of hyperbilirubinemia in healthy full-term newborn infants.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>8</FONT></U></A> </SUP>
<LI>The most rapid way to reduce the bilirubin level is to interrupt breastfeeding for 24 hours, feed with formula, and use phototherapy; however, in most infants, interrupting breastfeeding is not necessary or advisable.
<LI>Phototherapy can be administered with standard phototherapy units and fiberoptic blankets.<BR><BR>
<DIV class=emedinlineimage>
<BLOCKQUOTE><A href="javascript:showcontent('active','hiddenlayerd26e1107');"><IMG alt="The graph represents indications for phototherapy..." src="https://img1.daumcdn.net/relay/cafe/original/?fname=http%3A%2F%2Fimg.medscape.com%2Fpi%2Femed%2Fckb%2Fpediatrics_cardiac%2F1331339-1331345-973629-1769964tn.jpg"></A>
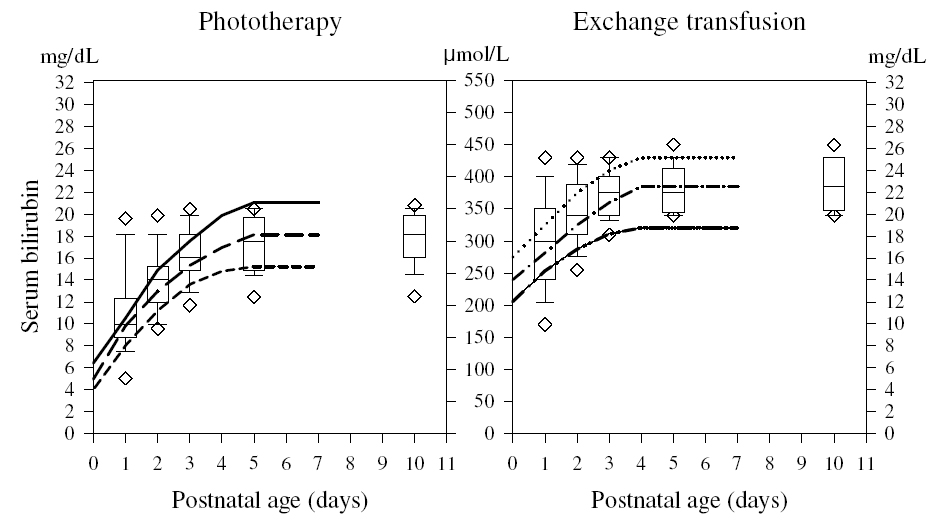
<H4>The graph represents indications for phototherapy and exchange transfusion in infants (with a birthweight of 3500 g) in 108 neonatal ICUs. The left panel shows the range of indications for phototherapy, whereas the right panel shows the indications for exchange transfusion. Numbers on the vertical axes are serum bilirubin concentrations in mg/dL (lateral) and mmol/L (middle). In the left panel, the solid line refers to the current recommendation of the American Academy of Pediatrics (AAP) for low-risk infants, the line consisting of long dashes (- - - - -) represents the level at which the AAP recommends phototherapy for infants at intermediate risk, and the line with short dashes (-----) represents the suggested intervention level for infants at high risk. In the right panel, the dotted line (......) represents the AAP suggested intervention level for exchange transfusion in infants considered at low risk, the line consisting of dash-dot-dash (-.-.-.-.) represents the suggested intervention level for exchange transfusion in infants at intermediate risk, and the line consisting of dash-dot-dot-dash (-..-..-..-) represents the suggested intervention level for infants at high risk. Intensive phototherapy is always recommended while preparations for exchange transfusion are in progress. The box-and-whisker plots show the following values: lower error bar = 10th percentile; lower box margin = 25th percentile; line transecting box = median; upper box margin = 75th percentile; upper error bar = 90th percentile; and lower and upper diamonds = 5th and 95th percentiles, respectively.</H4></BLOCKQUOTE></DIV>
<DIV class=inactive id=hiddenlayerd26e1107>
<DIV class=layerbg>
<DIV class=closewindow>[ <A href="javascript:showcontent('inactive','hiddenlayerd26e1107');"><U><FONT color=#004276>CLOSE WINDOW</FONT></U></A> ]</DIV>
<BLOCKQUOTE><IMG height=520 alt="The graph represents indications for phototherapy..." src="https://img1.daumcdn.net/relay/cafe/original/?fname=http%3A%2F%2Fimg.medscape.com%2Fpi%2Femed%2Fckb%2Fpediatrics_cardiac%2F1331339-1331345-973629-1769964.jpg" width=948 border=1></BLOCKQUOTE>
<H4>The graph represents indications for phototherapy and exchange transfusion in infants (with a birthweight of 3500 g) in 108 neonatal ICUs. The left panel shows the range of indications for phototherapy, whereas the right panel shows the indications for exchange transfusion. Numbers on the vertical axes are serum bilirubin concentrations in mg/dL (lateral) and mmol/L (middle). In the left panel, the solid line refers to the current recommendation of the American Academy of Pediatrics (AAP) for low-risk infants, the line consisting of long dashes (- - - - -) represents the level at which the AAP recommends phototherapy for infants at intermediate risk, and the line with short dashes (-----) represents the suggested intervention level for infants at high risk. In the right panel, the dotted line (......) represents the AAP suggested intervention level for exchange transfusion in infants considered at low risk, the line consisting of dash-dot-dash (-.-.-.-.) represents the suggested intervention level for exchange transfusion in infants at intermediate risk, and the line consisting of dash-dot-dot-dash (-..-..-..-) represents the suggested intervention level for infants at high risk. Intensive phototherapy is always recommended while preparations for exchange transfusion are in progress. The box-and-whisker plots show the following values: lower error bar = 10th percentile; lower box margin = 25th percentile; line transecting box = median; upper box margin = 75th percentile; upper error bar = 90th percentile; and lower and upper diamonds = 5th and 95th percentiles, respectively.</H4></DIV></DIV><BR>
<UL>
<LI>Fiberoptic phototherapy can often be safely administered at home, which may allow for improved infant-maternal bonding.
<LI>Although sunlight provides sufficient irradiance in the 425-nm to 475-nm band to provide phototherapy, practical difficulties involved in safely exposing a naked newborn to sunlight, either indoors or outdoors (and avoiding sunburn), preclude the use of sunlight as a reliable phototherapy tool; therefore, it is not recommended.
<LI>Phototherapy can be discontinued when serum bilirubin levels drop to less than 15 mg/dL (260 ?mol/L).
<LI>Average bilirubin level rebound has been shown to be less than 1 mg/dL (17 ?mol/L); therefore, rechecking the level after discontinuation of phototherapy is not necessary unless hyperbilirubinemia is due to a hemolytic process.
<LI>For an in-depth discussion of phototherapy, see <A href="http://emedicine.medscape.com/article/974786-overview" target="_blank"><U><FONT color=#004276>Jaundice, Neonatal</FONT></U></A>.</LI></UL></LI></UL></DIV><A name=1129></A>
<H3>Consultations</H3><A id=TreatmentConsultations name=TreatmentConsultations></A>
<UL>
<LI>Consider consultation with a neonatologist when serum bilirubin level approaches 20 mg/dL (430 ?mol/L) or when signs and symptoms suggest pathological jaundice and the rate of rise in the serum bilirubin level is more than 0.5 mg/dL/h.
<LI>A consultation with a lactation specialist is recommended in any breastfed baby who has jaundice. The expertise of lactation consultants can be extremely helpful, especially in situations in which inadequate breastfeeding is contributing to the jaundice.</LI></UL><A name=1130></A>
<H3>Diet</H3><A id=TreatmentDiet name=TreatmentDiet></A>
<UL>
<LI>Continue breastfeeding, if possible, and increase frequency of feeding to 8-12 times per day.
<LI>Depending on maternal preference, breastfeeding can be supplemented or replaced by formula at the same frequency. Supplementation with dextrose solution is not recommended because it may decrease caloric intake and milk production and may consequently delay the drop in serum bilirubin concentration. Breastfeeding can also be supplemented by pumped breast milk.</LI></UL><A name=1131></A>
<H3>Activity</H3><A id=TreatmentActivity name=TreatmentActivity></A>
<UL>
<LI>No restrictions are necessary.
<LI>Encourage parents to remove the child from the warmer or infant crib for feeding and bonding. Fiberoptic blankets allow holding and breastfeeding without interruption in treatment.</LI></UL><A name=18></A>
<H2>Medication</H2><A id=MEDICATION name=MEDICATION></A>
<UL>
<LI>Medication is not currently a component of care in this condition. See <A href="http://emedicine.medscape.com/article/973629-treatment#Treatment"><U><FONT color=#5757a6>Treatment</FONT></U></A>.</LI></UL><A name=26></A>
<H2>Follow-up</H2><A id=Followup name=Followup></A><A name=2644></A>
<H3>Further Inpatient Care</H3><A id=FollowupFurtherInpatientCare name=FollowupFurtherInpatientCare></A>
<DIV>
<UL>
<LI>If the patient has not been discharged with the parent, monitoring daily weights and serum bilirubin concentration for the need for phototherapy as well as assessment of caloric intake are important. Once serum bilirubin concentration is determined to be within a safe range (<20 mg/dL) and is not rapidly rising, home phototherapy is an option to consider as long as thorough outpatient follow-up (home visiting nursing assessment or office check-up and bilirubin level monitoring) are feasible.<A id=weightmonitoring name=weightmonitoring><U> </U></A>
<LI>Weight monitoring is very important in breastfed infants to avoid prolonged and severe jaundice, as well as to avoid hypernatremic dehydration. The general standard states that loss of 10% of birth weight is considered to be significant.
<LI>A reference chart for relative weight change to detect hypernatremic dehydration has been proposed.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>9</FONT></U></A> </SUP></LI></UL></DIV><A name=2645></A>
<H3>Further Outpatient Care</H3><A id=FollowupFurtherOutpatientCare name=FollowupFurtherOutpatientCare></A>
<UL>
<LI>If the infant is treated on an outpatient basis, measure serum bilirubin levels daily either in the clinic or in the home with home-health nurses until the bilirubin level is less than 15 mg/dL (260 ?mol/L).</LI></UL><A name=2647></A>
<H3>Transfer</H3><A id=FollowupTransfer name=FollowupTransfer></A>
<UL>
<LI>Transfer infants with pathologic jaundice or bilirubin levels greater than 20 mg/dL to a center capable of performing exchange transfusions.</LI></UL><A name=2648></A>
<H3>Deterrence/Prevention</H3><A id=FollowupDeterrencePrevention name=FollowupDeterrencePrevention></A>
<UL>
<LI>Poor caloric intake associated with insufficient breastfeeding contributes to the development of severe breast milk jaundice (BMJ). The first step toward successful breastfeeding is to make sure that mothers nurse their infants at least 8-12 times per day for the first several days starting from the first hour of life. The whey portion of human milk contains a feedback inhibitory peptide of lactogenesis; hence, effective emptying of the breast with each feeding results in successful lactation.
<LI>Infants who nursed more than 8 times during the first 24 hours had earlier meconium passage, reduced maximum weight loss, increased breast milk intake on days 3 and 5, and lower serum bilirubin levels and significantly lower incidence of severe hyperbilirubinemia (>15 mg/dL) on day 6.
<LI>In a recent double-blind controlled study, beta-glucuronidase inhibition with L-aspartic acid and enzymatically hydrolyzed casein in exclusively breastfed babies resulted in reduction in peak serum bilirubin level by 70% in first week of life.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>10</FONT></U></A> </SUP>
<LI>According to the latest clinical practice guidelines for the management of hyperbilirubinemia in the newborn aged 35 or more weeks' gestation, exclusive breastfeeding is a major risk factor for severe hyperbilirubinemia and all infants should be eval‎!uated for the risk of subsequent hyperbilirubinemia by plotting their discharge serum bilirubin levels on an hour-specific nomogram.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>8</FONT></U></A> </SUP>.<A id=combinationrisk name=combinationrisk><U> </U></A>
<LI>Transcutaneous bilirubinometry is a measurement of yellow color of the blanched skin and subcutaneous tissue and can be used as a screening tool. It has been shown to be fairly reliable, with good correlation between total serum bilirubin (TSB) and transcutaneous bilirubin (TcB) levels obtained using instruments currently available in the United States (eg, Draeger Air-Shields Jaundice Meter JM-103, Respironics BiliChek meter by Philips). The TcB measurement tends to underestimate the TSB at higher levels.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>11</FONT></U></A> </SUP>Confirm‎!ation with TSB measurement is indicated in all patients with TcB levels above the 75th percentile and in those in whom therapeutic intervention is considered.
<LI>Recent studies suggest that combining clinical risk factors with predischarge measurement of TSB or TcB levels improves the accuracy of risk assessment for subsequent hyperbilirubinemia.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>12</FONT></U></A> </SUP>The factors most predictive included predischarge TSB or TcB levels above 75th percentile, lower gestational age, and exclusive breastfeeding.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>13</FONT></U></A> </SUP>
<LI>Newborns who are exclusively breastfed and who have elevated predischarge TcB or TSB levels do not qualify for discharge before 48 hours and should be eval‎!uated for phototherapy in 24 hours. Newborns with TcB and TSB levels in the high-intermediate range and newborns who were born at less than 38 weeks' gestation should undergo repeat TSB and TcB measurement within 24 hours of discharge or should receive follow-up within 2 days.<SUP><A href="javascript:showcontent('active','references');"><U><FONT color=#004276>14</FONT></U></A> </SUP></LI></UL><A name=2649></A>
<H3>Complications</H3><A id=FollowupComplications name=FollowupComplications></A>
<UL>
<LI>Bilirubin encephalopathy (kernicterus) may occur in exclusively breastfed infants in the absence of hemolysis or other specific pathologic conditions.
<LI>Distinguishing between breastfeeding jaundice and breast milk jaundice is important because bilirubin-induced encephalopathy occurs more commonly in breastfeeding jaundice.
<LI>Near-term infants (35-37 weeks' gestation) are more likely to manifest breastfeeding jaundice because of difficulty achieving adequate nursing, greater weight loss, and hepatic immaturity.</LI></UL><A name=2650></A>
<H3>Prognosis</H3><A id=FollowupPrognosis name=FollowupPrognosis></A>
<UL>
<LI>Prognosis is excellent, although jaundice in breastfed infants may persist for as long as 12 weeks.</LI></UL><A name=2651></A>
<H3>Patient Education</H3><A id=FollowupPatientEducation name=FollowupPatientEducation></A>
<UL>
<LI>Provide excellent breastfeeding education. Refer to a lactation consultant or La Leche League.
<LI>For excellent patient education resources, visit eMedicine's <A href="http://www.emedicinehealth.com/collections/CO1602.asp" target=_blank><U><FONT color=#004276>Pregnancy and Reproduction Center</FONT></U></A>. Also, see eMedicine's patient education article <A href="http://www.emedicinehealth.com/articles/12156-1.asp" target=_blank><U><FONT color=#004276>Breastfeeding</FONT></U></A>.</LI></UL><A name=27></A>
<H2>Miscellaneous</H2><A id=Miscellaneous name=Miscellaneous></A><A name=2752></A>
<H3>Medicolegal Pitfalls</H3><A id=MiscellaneousMedicalLegalPitfalls name=MiscellaneousMedicalLegalPitfalls></A>
<UL>
<LI>Failure to differentiate breast milk jaundice (BMJ) from pathologic jaundice
<LI>Failure to appropriately treat elevated bilirubin levels in a timely manner
<LI>Failure to identify and treat inadequate breastfeeding, with resultant dehydration</LI></UL><A name=2753></A>
<H3>Special Concerns</H3><A id=MiscellaneousSpecialConcerns name=MiscellaneousSpecialConcerns></A>
<UL>
<LI>Treat preterm infants (estimated gestational age <37 wk at birth) with phototherapy at lower bilirubin levels (see <A href="http://emedicine.medscape.com/article/974786-overview" target="_blank"><U><FONT color=#004276>Jaundice, Neonatal</FONT></U></A>).</LI></UL>
<P>from (<A href="http://emedicine.medscape.com/article/973629-followup" target="_blank">http://emedicine.medscape.com/article/973629-followup</A>)</P>
<!-- -->
Arias first described breast milk jaundice (BMJ) in 1963. Breast milk jaundice is a type of neonatal jaundice associated with breastfeeding. It is characterized by indirect hyperbilirubinemia in a breastfed newborn that develops after the first 4-7 days of life, persists longer than physiologic jaundice, and has no other identifiable cause. It should be differentiated from breastfeeding jaundice, which manifests in the first week of life and is caused by insufficient production or intake of breast milk.
Pathophysiology
The etiology of breast milk jaundice is not clearly understood, but the following factors have been suggested to play a role:
An unusual metabolite of progesterone (pregnane-3-alpha 20 beta-diol), a substance in the breast milk that inhibits uridine diphosphoglucuronic acid (UDPGA) glucuronyl transferase
Increased concentrations of nonesterified free fatty acids that inhibit hepatic glucuronyl transferase
Increased enterohepatic circulation of bilirubin due to (1) increased content of beta glucuronidase activity in breast milk and, therefore, the intestines of the breastfed neonate and (2) delayed establishment of enteric flora in breastfed infants
Defects in uridine diphosphate-glucuronyl transferase (UGT1A1) activity in infants who are homozygous or heterozygous for variants of the Gilbert syndrome promoter and coding region polymorphism.
Reduced hepatic uptake of unconjugated bilirubin due to a mutation in the solute carrier organic anion transporter protein SLCO1B1.
Inflammatory cytokines in human milk, especially interleukin (IL)-1 beta and IL-6, are increased in individuals with breast milk jaundice and are known to be cholestatic and reduce the uptake, metabolism, and excretion of bilirubin.1
High epidermal growth factor (EGF) levels in breast milk may be responsible for jaundice in these neonates. EGF is responsible for growth, proliferation, and maturation of the GI tract in newborns and is vital for is adaptation after birth. Higher EGF serum and breast milk levels were noted in patients with breast milk jaundice.2The reduced GI motility and increased bilirubin absorption and uptake are thought to be the mechanisms.
Please see Jaundice, Neonatal for an in-depth review of the pathophysiology of hyperbilirubinemia.
Frequency
United States
Jaundice occurs in 50-70% of newborns. Moderate jaundice (bilirubin level >12 mg/dL) develops in 4% of bottle-fed newborns, compared to 14% of breastfed newborns. Severe jaundice (bilirubin level >15 mg/dL) occurs in 0.3% of bottle-fed newborns, compared to 2% of breastfed newborns. A strong familial predisposition is also suggested by the recurrence of breast milk jaundice in siblings.
International
International frequency is not extensively reported but is thought to be similar to that in the United States.
Mortality/Morbidity
Breast milk jaundice in otherwise healthy full-term infants rarely causes kernicterus (bilirubin encephalopathy). Case reports suggest that some breastfed infants who suffer from prolonged periods of inadequate breast milk intake and whose bilirubin levels exceeded 25 mg/dL may be at risk of kernicterus. Another group of breastfed infants who may be at risk of complications are borderline premature infants (36-37 weeks' gestational age) who are poorly nursing.
Race
Whether racial differences are observed in breast milk jaundice is unclear, although an increased preval!ence of physiologic jaundice is observed in babies of Chinese, Japanese, Korean, and Native American descent.
Sex
No sex predilection is known.
Age
Breast milk jaundice manifests after the first 4-7 days of life and can persist for 3-12 weeks.
Clinical
History
Physiologic jaundice usually manifests after the first 24 hours of life. This can be accentuated by breastfeeding, which, in the first few days of life, may be associated with suboptimal milk and suboptimal caloric intake, especially if milk production is delayed. This is known as breastfeeding jaundice. Jaundice that manifests before the first 24 hours of life should always be considered pathologic until proven otherwise. In this situation, a full diagnostic workup with emphasis on infection and hemolysis should be undertaken.
True breast milk jaundice (BMJ) manifests after the first 4-7 days of life. A second peak in serum bilirubin level is noted by age 14 days.
In clinical practice, differentiating between physiologic jaundice from breast milk jaundice is important so that the duration of hyperbilirubinemia can be predicted. Identifying the infants who become dehydrated secondary to inadequate breastfeeding is also important. These babies need to be identified early and given breastfeeding support and formula supplementation as necessary. Depending on serum bilirubin concentration, neonates with hyperbilirubinemia may become sleepy and feed poorly.
Physical
Clinical jaundice is usually first noticed in the sclera and the face. Then it progresses caudally to reach the abdomen and extremities. Gentle pressure on the skin helps to reveal the extent of jaundice, especially in darker-skinned babies; however, clinical observation is not an accurate measure of the severity of the hyperbilirubinemia.
A rough correlation is observed between blood levels and the extent of jaundice (face, approximately 5 mg/dL; mid abdomen, approximately 15 mg/dL; soles, 20 mg/dL). Therefore, clinical decisions should always be based on serum levels of bilirubin. Skin should have normal perfusion and turgor and show no petechiae.
Neurologic examination, including neonatal reflexes, should be normal, although the infant may be sleepy. Muscle tone and reflexes (eg, Moro reflex, grasp, rooting) should be normal.
Eval!uate hydration status by an assessment of the percentage of birth weight that may have been lost, observation of mucous membranes, fontanelle, and skin turgor.
Causes
Supplementation of breastfeeding with dextrose 5% in water (D5W) can actually increase the preval!ence or degree of jaundice.
Delayed milk production and poor feeding lead to decreased caloric intake, dehydration, and increased enterohepatic circulation, resulting in higher serum bilirubin concentration.
The biochemical cause of breast milk jaundice remains under investigation. Some research reported that lipoprotein lipase, found in some breast milk, produces nonesterified long-chain fatty acids, which competitively inhibit glucuronyl transferase conjugating activity.
Glucuronidase has also been found in some breast milk, which results in jaundice.
Decreased uridine diphosphate-glucuronyl transferase (UGT1A1) activity may be associated with prolonged hyperbilirubinemia in breast milk jaundice.3This may be comparable to what is observed in patients with Gilbert syndrome.4Genetic polymorphisms of the UGT1A1 promoter, specifically the T-3279G and the thymidine-adenine (TA)7 dinucleotide repeat TATAA box variants, were found to be commonly inherited in whites with high allele frequency. These variant promoters reduce the transcriptional UGT1A1 activity. Similarly, mutations in the coding region of the UGT1A1 (eg, G211A, C686A, C1091T, T1456G) have been described in East Asian populations; these mutations reduce the activity of the enzyme and are a cause of Gilbert syndrome.5
The G211A mutation in exon 1 (Gly71Arg) is most common, with an allele frequency of 13%. Coexpression! of these polymorphism in the promoter and in the coding region are common and further impair the enzyme activity.6
Hepatic solute carrier organic anion transporter 1B1 (SLCO1B1) is a sinusoidal membrane protein involved in uptake of unconjugated bilirubin. Mutation of the gene for SLCO1B1, namely the A388G missense variant, was associated with increased risk of neonatal hyperbilirubinemia with exclusive breast feeding.7
Hemolytic anemia (RBC membrane defects: spherocytosis, acanthocytosis, ovalocytosis; RBC enzyme defects, hemoglobinopathies) Blood type incompatibility (ABO and minor group antigens) Large cephalhematoma Hypothyroidism Urinary tract infections Sepsis Gilbert syndrome Early galactosemia
Workup
Laboratory Studies
Breast milk jaundice (BMJ) is a diagnosis of exclusion. Detailed history and physical examination showing that the infant is thriving and that lactation is well established are key elements to diagnosis. Breastfed babies should have 3-4 transitional stools and 6-7 wet diapers per day and should have regained birth weight by the end of the second week of life or demonstrate a weight gain of 1 oz/d.
Measure total serum bilirubin concentration in neonates who have jaundice that has progressed from the face to the chest and in neonates at risk for hemolytic disease of the newborn.
The following tests are to be considered if serum bilirubin levels are greater than 12 mg/dL (170 ?mol/L). A total serum bilirubin concentration that rises faster than 5 mg/dL/d (85 ?mol/L/d) or jaundice before 24 hours of life suggests pathologic jaundice.
Sepsis (WBC count, <5 K/mL or >20 K/mL) with immature to total neutrophil ratio greater than 0.2
Urine specific gravity can be useful in the assessment of hydration status.
If hemolysis is suspected, consider the following tests:
Blood type to eval!uate for ABO, Rh or other blood group incompatibility
Coombs test, as well as an elution test for antibodies against A or B, to eval!uate for immune mediated hemolysis
Peripheral smear to look for abnormally shaped RBCs (ovalocytes, acanthocytes, spherocytes, schistocytes)
Glucose-6-phosphate dehydrogenase (G-6-PD) screen, especially if ethnicity consistent
Factors that suggest possibility of hemolytic disease include the following:
Family history of hemolytic disease
Onset of jaundice before 24 hours of life
Rise in serum bilirubin levels of more than 0.5 mg/dL/h
Pallor, hepatosplenomegaly
Rapid increase in serum bilirubin level after 24-48 hours (G-6-PD deficiency)
Ethnicity suggestive of G-6-PD deficiency
Failure of phototherapy to lower bilirubin level
If sepsis is suspected, consider the following tests:
Blood culture
WBC differential
Platelet count
Urine analysis and culture
Factors that suggest the possibility of sepsis include the following:
Poor feeding
Vomiting
Lethargy
Temperature instability
Apnea
Tachypnea
Signs of cholestatic jaundice that suggest the need to rule out biliary atresia or other causes of cholestasis include the following:
Dark urine or urine positive for bilirubin
Light-colored stools
Persistent jaundice for more than 3 weeks
The follow-up includes the state newborn screen for galactosemia and hypothyroidism.
Treatment
Medical Care
Treatment recommendations in this section apply only to healthy term infants with no signs of pathologic jaundice and are based on the severity of hyperbilirubinemia. In preterm, anemic, or ill infants and those with early (<24 h) or severe jaundice (>25 mg/dL or 430 ?mol/L), different treatment protocols should be pursued (see Jaundice, Neonatal).
For healthy term infants with breast milk or breastfeeding jaundice and with bilirubin levels of 12 mg/dL (170 ?mol/L) to 17 mg/dL, the following options are acceptable:
Increase breastfeeding to 8-12 times per day and recheck the serum bilirubin level in 12-24 hours. The mother should be reassured about the relatively benign nature of breast milk jaundice (BMJ). This recommendation assumes that effective breastfeeding is occurring, including milk production, effective latching, and effective sucking with resultant letdown of milk. Breastfeeding can also be supported with manual or electric pumps and the pumped milk given as a supplement to the baby.
Continue breastfeeding and supplement with formula.
Temporary interruption of breastfeeding is rarely needed and is not recommended unless serum bilirubin levels reach 20 mg/dL (340 ?mol/L).
For infants with serum bilirubin levels from 17-25 mg/dL (294-430 ?mol/L), add phototherapy to any of the previously stated treatment options. The reader is referred to the American Academy of Pediatrics' practice parameter on the management of hyperbilirubinemia in healthy full-term newborn infants.8
The most rapid way to reduce the bilirubin level is to interrupt breastfeeding for 24 hours, feed with formula, and use phototherapy; however, in most infants, interrupting breastfeeding is not necessary or advisable.
Phototherapy can be administered with standard phototherapy units and fiberoptic blankets.
The graph represents indications for phototherapy and exchange transfusion in infants (with a birthweight of 3500 g) in 108 neonatal ICUs. The left panel shows the range of indications for phototherapy, whereas the right panel shows the indications for exchange transfusion. Numbers on the vertical axes are serum bilirubin concentrations in mg/dL (lateral) and mmol/L (middle). In the left panel, the solid line refers to the current recommendation of the American Academy of Pediatrics (AAP) for low-risk infants, the line consisting of long dashes (- - - - -) represents the level at which the AAP recommends phototherapy for infants at intermediate risk, and the line with short dashes (-----) represents the suggested intervention level for infants at high risk. In the right panel, the dotted line (......) represents the AAP suggested intervention level for exchange transfusion in infants considered at low risk, the line consisting of dash-dot-dash (-.-.-.-.) represents the suggested intervention level for exchange transfusion in infants at intermediate risk, and the line consisting of dash-dot-dot-dash (-..-..-..-) represents the suggested intervention level for infants at high risk. Intensive phototherapy is always recommended while preparations for exchange transfusion are in progress. The box-and-whisker plots show the following values: lower error bar = 10th percentile; lower box margin = 25th percentile; line transecting box = median; upper box margin = 75th percentile; upper error bar = 90th percentile; and lower and upper diamonds = 5th and 95th percentiles, respectively.
The graph represents indications for phototherapy and exchange transfusion in infants (with a birthweight of 3500 g) in 108 neonatal ICUs. The left panel shows the range of indications for phototherapy, whereas the right panel shows the indications for exchange transfusion. Numbers on the vertical axes are serum bilirubin concentrations in mg/dL (lateral) and mmol/L (middle). In the left panel, the solid line refers to the current recommendation of the American Academy of Pediatrics (AAP) for low-risk infants, the line consisting of long dashes (- - - - -) represents the level at which the AAP recommends phototherapy for infants at intermediate risk, and the line with short dashes (-----) represents the suggested intervention level for infants at high risk. In the right panel, the dotted line (......) represents the AAP suggested intervention level for exchange transfusion in infants considered at low risk, the line consisting of dash-dot-dash (-.-.-.-.) represents the suggested intervention level for exchange transfusion in infants at intermediate risk, and the line consisting of dash-dot-dot-dash (-..-..-..-) represents the suggested intervention level for infants at high risk. Intensive phototherapy is always recommended while preparations for exchange transfusion are in progress. The box-and-whisker plots show the following values: lower error bar = 10th percentile; lower box margin = 25th percentile; line transecting box = median; upper box margin = 75th percentile; upper error bar = 90th percentile; and lower and upper diamonds = 5th and 95th percentiles, respectively.
Fiberoptic phototherapy can often be safely administered at home, which may allow for improved infant-maternal bonding.
Although sunlight provides sufficient irradiance in the 425-nm to 475-nm band to provide phototherapy, practical difficulties involved in safely exposing a naked newborn to sunlight, either indoors or outdoors (and avoiding sunburn), preclude the use of sunlight as a reliable phototherapy tool; therefore, it is not recommended.
Phototherapy can be discontinued when serum bilirubin levels drop to less than 15 mg/dL (260 ?mol/L).
Average bilirubin level rebound has been shown to be less than 1 mg/dL (17 ?mol/L); therefore, rechecking the level after discontinuation of phototherapy is not necessary unless hyperbilirubinemia is due to a hemolytic process.
Consider consultation with a neonatologist when serum bilirubin level approaches 20 mg/dL (430 ?mol/L) or when signs and symptoms suggest pathological jaundice and the rate of rise in the serum bilirubin level is more than 0.5 mg/dL/h.
A consultation with a lactation specialist is recommended in any breastfed baby who has jaundice. The expertise of lactation consultants can be extremely helpful, especially in situations in which inadequate breastfeeding is contributing to the jaundice.
Diet
Continue breastfeeding, if possible, and increase frequency of feeding to 8-12 times per day.
Depending on maternal preference, breastfeeding can be supplemented or replaced by formula at the same frequency. Supplementation with dextrose solution is not recommended because it may decrease caloric intake and milk production and may consequently delay the drop in serum bilirubin concentration. Breastfeeding can also be supplemented by pumped breast milk.
Activity
No restrictions are necessary.
Encourage parents to remove the child from the warmer or infant crib for feeding and bonding. Fiberoptic blankets allow holding and breastfeeding without interruption in treatment.
Medication
Medication is not currently a component of care in this condition. See Treatment.
Follow-up
Further Inpatient Care
If the patient has not been discharged with the parent, monitoring daily weights and serum bilirubin concentration for the need for phototherapy as well as assessment of caloric intake are important. Once serum bilirubin concentration is determined to be within a safe range (<20 mg/dL) and is not rapidly rising, home phototherapy is an option to consider as long as thorough outpatient follow-up (home visiting nursing assessment or office check-up and bilirubin level monitoring) are feasible.
Weight monitoring is very important in breastfed infants to avoid prolonged and severe jaundice, as well as to avoid hypernatremic dehydration. The general standard states that loss of 10% of birth weight is considered to be significant.
A reference chart for relative weight change to detect hypernatremic dehydration has been proposed.9
Further Outpatient Care
If the infant is treated on an outpatient basis, measure serum bilirubin levels daily either in the clinic or in the home with home-health nurses until the bilirubin level is less than 15 mg/dL (260 ?mol/L).
Transfer
Transfer infants with pathologic jaundice or bilirubin levels greater than 20 mg/dL to a center capable of performing exchange transfusions.
Deterrence/Prevention
Poor caloric intake associated with insufficient breastfeeding contributes to the development of severe breast milk jaundice (BMJ). The first step toward successful breastfeeding is to make sure that mothers nurse their infants at least 8-12 times per day for the first several days starting from the first hour of life. The whey portion of human milk contains a feedback inhibitory peptide of lactogenesis; hence, effective emptying of the breast with each feeding results in successful lactation.
Infants who nursed more than 8 times during the first 24 hours had earlier meconium passage, reduced maximum weight loss, increased breast milk intake on days 3 and 5, and lower serum bilirubin levels and significantly lower incidence of severe hyperbilirubinemia (>15 mg/dL) on day 6.
In a recent double-blind controlled study, beta-glucuronidase inhibition with L-aspartic acid and enzymatically hydrolyzed casein in exclusively breastfed babies resulted in reduction in peak serum bilirubin level by 70% in first week of life.10
According to the latest clinical practice guidelines for the management of hyperbilirubinemia in the newborn aged 35 or more weeks' gestation, exclusive breastfeeding is a major risk factor for severe hyperbilirubinemia and all infants should be eval!uated for the risk of subsequent hyperbilirubinemia by plotting their discharge serum bilirubin levels on an hour-specific nomogram.8.
Transcutaneous bilirubinometry is a measurement of yellow color of the blanched skin and subcutaneous tissue and can be used as a screening tool. It has been shown to be fairly reliable, with good correlation between total serum bilirubin (TSB) and transcutaneous bilirubin (TcB) levels obtained using instruments currently available in the United States (eg, Draeger Air-Shields Jaundice Meter JM-103, Respironics BiliChek meter by Philips). The TcB measurement tends to underestimate the TSB at higher levels.11Confirm!ation with TSB measurement is indicated in all patients with TcB levels above the 75th percentile and in those in whom therapeutic intervention is considered.
Recent studies suggest that combining clinical risk factors with predischarge measurement of TSB or TcB levels improves the accuracy of risk assessment for subsequent hyperbilirubinemia.12The factors most predictive included predischarge TSB or TcB levels above 75th percentile, lower gestational age, and exclusive breastfeeding.13
Newborns who are exclusively breastfed and who have elevated predischarge TcB or TSB levels do not qualify for discharge before 48 hours and should be eval!uated for phototherapy in 24 hours. Newborns with TcB and TSB levels in the high-intermediate range and newborns who were born at less than 38 weeks' gestation should undergo repeat TSB and TcB measurement within 24 hours of discharge or should receive follow-up within 2 days.14
Complications
Bilirubin encephalopathy (kernicterus) may occur in exclusively breastfed infants in the absence of hemolysis or other specific pathologic conditions.
Distinguishing between breastfeeding jaundice and breast milk jaundice is important because bilirubin-induced encephalopathy occurs more commonly in breastfeeding jaundice.
Near-term infants (35-37 weeks' gestation) are more likely to manifest breastfeeding jaundice because of difficulty achieving adequate nursing, greater weight loss, and hepatic immaturity.
Prognosis
Prognosis is excellent, although jaundice in breastfed infants may persist for as long as 12 weeks.
Patient Education
Provide excellent breastfeeding education. Refer to a lactation consultant or La Leche League.